| QUICK ANSWER Provider credentialing typically takes 90 to 150 days, from the initial application to payer approval. The timeline varies by stage: CAQH setup takes 1 to 2 weeks, primary source verification takes 2 to 4 weeks, and payer enrollment can take 60 to 120 days, depending on the payer. Hospital privileging, when required, can add another 30 to 90 days. The most common causes of delays are incomplete applications, outdated documentation, and payer backlogs. |
Every day a provider spends on credentialing is a day they cannot bill. That is not an intellectual concern. It is a real, measurable revenue gap that compounds across every provider in a practice, every payer they need to enroll with, and each day the process runs longer than it should.
Provider credentialing refers to the process of verification and enrollment that insurance payers need before provider’s claim submissions and receive reimbursement. Without it, a provider can treat patients but cannot get paid by that payer’s network. For any practice that relies on insurance reimbursement, credentialing is not an optional infrastructure, but the gateway to revenue.
This guide walks you through all the stages of the complete credentialing timeline. It covers what each phase includes, what usually causes delays, and what credentialing teams can do to move sooner without skipping steps.
What Is Provider Credentialing?
Provider credentialing is the process by which healthcare organizations and insurance payers verify a provider’s qualifications before authorizing them to treat patients under a given insurance plan and bill for those services. It covers academic credentials, medical licenses, board certifications, malpractice history, work history, and background checks.
Three terms are often used interchangeably in this space, but they serve different purposes:
| Term | What It Actually Means |
| Credentialing | Verification of a provider’s qualifications by a payer or healthcare organization. |
| Provider Enrollment | The administrative process of enrolling a credentialed provider into a payer’s network so they can bill. Often used interchangeably with credentialing. |
| Privileging | A hospital-specific process granting a provider permission to perform certain procedures at that facility. Follows credentialing and is separate from payer enrollment. |
In practice, when a credentialing manager says they are credentialing a provider, they typically mean both verifying qualifications and completing payer enrollment at the same time. For the purposes of this guide, credentialing refers to the complete end-to-end process.
The Centers for Medicare and Medicaid Services (CMS) sets overarching regulatory standards, while individual payers, numbering over 34,000 across the United States, each operate their own enrollment requirements. That fragmentation is precisely why credentialing takes as long as it does.
How Long Does Provider Credentialing Take?
| QUICK ANSWEROn average, provider credentialing takes 90 to 150 days from start to approval. Commercial payers generally take 60 to 120 days. Medicare enrollment through PECOS typically runs 60 to 90 days. Medicaid timelines vary by state. Hospital privileging, when applicable, adds another 30 to 90 days on top of payer enrollment. |
The credentialing timeline is not a matter of one process, but numerous overlapping processes, each with its own dependencies and possible failure points. The table below breaks down the typical duration for each stage.
| Credentialing Stage | Typical Duration | Key Dependencies |
| CAQH Profile Setup and Attestation | 1 to 2 weeks | Provider accuracy, prior attestation status |
| Primary Source Verification (PSV) | 2 to 4 weeks | Institution response times |
| Payer Enrollment and Contracting | 60 to 120 days | Payer backlog, completeness of application |
| Hospital Privileging (if applicable) | 30 to 90 days | Committee meeting schedules |
| Re-credentialing (every 2 to 3 years) | 30 to 60 days | Currency of CAQH and supporting documents |
| NOTEThese timelines reflect typical ranges. Individual payers can fall well outside them depending on their current processing volumes, staffing, and internal review cycles. Some Medicare contractors process applications in 30 days. Some commercial payers routinely exceed 120 days during high-volume periods. |
One detail worth noting: A provider enrolling with a number of payers simultaneously does not stack these timelines. They run in parallel. But each payer is an individual workflow, and each one can fail individualistically, creating gaps that need individual follow-up.
Step-by-Step Provider Credentialing Process
Understanding where time is actually spent helps credentialing teams prioritize and plan. Here is a breakdown of each stage, what it involves, and where things tend to go wrong.
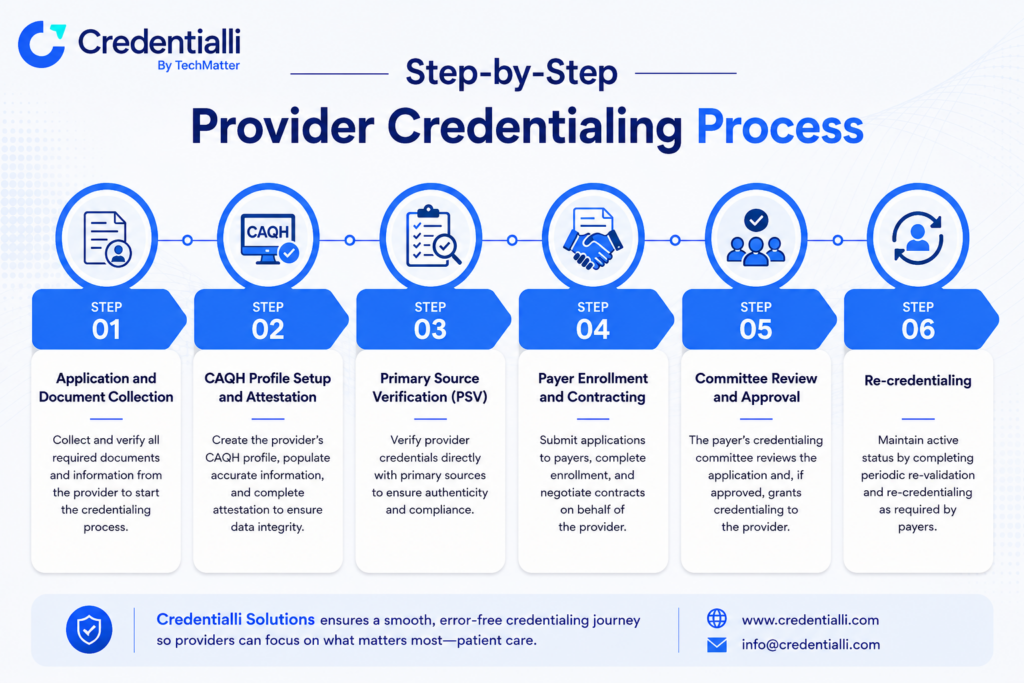
Step 1: Application and Document Collection
This is the foundation of everything that follows. Before any verification starts, the provider must submit a complete application package. This usually includes a current medical license, DEA certificate, NPI number (both the individual provider NPI and the practice NPI if billing under a group), board certifications, malpractice insurance certificates, a work history covering the past five to ten years, and any required background check authorizations.
The most common cause of delays at this stage is incomplete or inconsistent information. A name that appears differently on a license versus a diploma, an unexplained gap in work history, an expired malpractice certificate. Any of these can trigger a deficiency notice from the payer, which pauses the clock and restarts a review cycle.
| TIPReview the application for accuracy and completeness before submission, not after receiving a deficiency notice. A single missing field can add 4 to 6 weeks to the timeline. |
Step 2: CAQH Profile Setup and Attestation
CAQH, the Council for Affordable Quality Healthcare, operates ProView, a centralized database that most major commercial payers and many government payers use to retrieve provider information during enrollment. Rather than submitting documentation separately to each payer, a provider maintains a single CAQH profile that authorized payers can access.
Setting up a new CAQH profile takes roughly one to two weeks if all documentation is ready. Re-attestation, which CAQH requires every 120 days, is frequently overlooked. An expired CAQH profile can silently block payer access to provider data, causing delays that only surface weeks into an enrollment cycle.
For new providers, CAQH registration is typically one of the first steps. For existing providers adding new payer relationships, ensuring the CAQH profile is current and re-attested is equally critical.
Step 3: Primary Source Verification (PSV)
Primary source verification is the process of confirming credentials directly with the issuing organization rather than depending on copies provided by the provider. Medical school degrees are verified with the institution. Board certifications are confirmed with the certifying board. Licenses are verified with the state licensing authority. Malpractice history is pulled from the National Practitioner Data Bank (NPDB).
PSV typically takes two to four weeks, based on how quickly third-party organizations respond. State licensing boards and foreign medical schools are the most common sources of delay. International medical graduates face longer verification timelines due to extra steps required for foreign credential verification.
Many credentialing organizations use accredited PSV vendors to manage this process. Irrespective of who performs it, this is a non-negotiable step. No payer will complete enrollment without it.
Step 4: Payer Enrollment and Contracting
This is the longest stage of the process and the one with the least predictability. Once verification is complete, the credentialing manager submits formal enrollment applications to each payer. The payer’s credentialing committee reviews the application, confirms the PSV results, and determines whether to approve the provider for in-network status.
Most commercial payers take 60 to 120 days to complete this step. Medicare enrollment through PECOS typically takes 60 to 90 days. Medicaid timelines vary by state, ranging from 30 days in some states to well over 90 in others.
Throughout this period, the credentialing manager should follow up with each payer at regular intervals, typically every two to three weeks, to confirm receipt, check status, and address any outstanding items before they cause a formal rejection.
Step 5: Committee Review and Approval
Most payers organize a credentialing committee that reviews applications on a scheduled basis, sometimes monthly, sometimes quarterly. If an application misses a committee cycle, it waits for the next one. This scheduling dependency is one of the most frustrating sources of delay given that it has nothing to do with the quality or comprehensiveness of the application itself.
Once the committee approves the application, the payer issues an effective date for the provider to bill in-network. The effective date is oftentimes retroactive to the date the completed application was received, but this depends totally on the payer’s policy.
Step 6: Re-credentialing
Credentialing is not a one-time event. Payers require re-credentialing every two to three years. State licenses, DEA registrations, and malpractice insurance certificates all carry expiration dates. If any of these expire before re-credentialing is complete, the provider can be temporarily suspended from the payer’s network.
Many practices treat re-credentialing as lower priority than initial enrollment. Building a tracking system that monitors expiration dates and triggers re-credentialing workflows well in advance is one of the most impactful improvements a credentialing team can make.
Why Does Credentialing Take So Long?
The unsatisfying reality of the credentialing timeline is that most delays are not caused by the complexity of the process itself, but by operational failures such as missing information, poor tracking, missed follow-ups, and fragmented workflows spread across emails, spreadsheets, and multiple payer portals.
Here are the most common causes of credentialing delays, each of which is preventable with the right systems in place.
1. Incomplete or Inconsistent Applications
This is the single major source of avoidable delay. Payers have no obligation to chase down gaps. If a field is missing or information is inconsistent across documents, they issue a deficiency notice and pause the review. Depending on the payer’s processing cycle, this can add four to six weeks to the timeline.
2. CAQH Errors and Lapsed Attestations
An outdated CAQH profile is a silent delay. When a payer pulls provider data and finds expired or inconsistent information, they either pause the application or issue a deficiency. Because CAQH re-attestation is required every 120 days and many practices do not track it systematically, lapsed attestations are remarkably common. Industry surveys consistently identify CAQH maintenance as one of the top causes of enrollment delay.
3. Payer Backlogs and Slow Response Times
During high-volume periods, payers receive more applications than their credentialing teams can process quickly. Open enrollment periods, Medicaid expansion phases, and post-pandemic provider reentry cycles have all historically caused significant backlogs. There is little a credentialing team can do about this except start early and follow up consistently.
4. Manual Follow-Up and Lost Paperwork
When credentialing is managed through email and spreadsheets, follow-up depends entirely on human memory and calendar discipline. Applications sit unacknowledged. Payer contacts change. Documents get sent to the wrong address. Each of these becomes a delay that only surfaces when someone manually checks on an application that has been dormant for six weeks.
5. Expirables Caught Mid-Process
A license that expires during enrollment, a malpractice policy that lapses between submission and committee review, a DEA certificate that runs out before the payer finalizes approval. Any of these can pause or void an enrollment application. Providers and credentialing teams often do not realize the expiration has occurred until the payer flags it.
6. Poor Tracking Across Providers and Payers
For practices managing numerous providers across multiple payers, tracking enrollment status without a centralized system is genuinely difficult. When status lives in spreadsheets, updates are manual, and visibility relies on whoever last touched the file. Applications fall through the gaps. Deadlines get missed. By the time the problem surfaces, the delay has already compounded.
| INSIGHTA single credentialing coordinator managing 10 providers each enrolled with 15 payers is tracking 150 active applications simultaneously. Without structured workflows and automated tracking, the operational load makes consistent follow-up nearly impossible. |
How to Speed Up Provider Credentialing?
Most credentialing delays can be avoided successfully. The timeline cannot be compressed past the payer’s own internal processes, but a well-run credentialing operation can eradicate the compounding delays that occur before and around those processes.
Manual Best Practices that Make an Immediate Difference
- Submit complete applications the first time. Build a pre-submission checklist covering every required field, document, and certification. A rejection based on a missing field costs more time than the checklist saves.
- Keep CAQH current. Set a recurring calendar reminder for re-attestation at 100 days, not 120. By the time a notice arrives, the profile may already have expired.
- Start the process early. Credentialing takes time regardless of how well it is managed. Starting enrollment 90 to 120 days before a provider’s intended start date is standard practice. Starting earlier is better.
- Track expirables proactively. Maintain a master expiration calendar for licenses, certifications, DEA registrations, and malpractice policies. Flag anything expiring within 90 days for action.
- Designate a credentialing point of contact. Credentialing should not be someone’s secondary responsibility. Practices that assign a dedicated credentialing coordinator consistently outperform those that split the function across administrative staff.
- Follow up on a schedule. Establish a standing follow-up cadence with each payer, typically every two to three weeks. Do not wait for the payer to reach out.
Automate the Workflow
At a certain scale, manual credentialing becomes structurally unmaintainable. The processes that work for a two-provider practice do not hold up for a 20-provider group across multiple locations. Workflow automation addresses the root causes of delay directly:
- Centralized document management eliminates the problem of missing paperwork. All provider documents live in one place, with version control and audit trails. When a payer requests documentation, it is retrieved in minutes.
- Automated expiration monitoring removes the dependency on manual calendar tracking. The system flags documents approaching expiration and triggers a renewal workflow before the issue creates an enrollment problem.
- Multi-payer tracking from a single dashboard gives credentialing managers real-time visibility into every active application. Stalled applications are visible before they become critical.
- Linkage management handles the complexity of providers enrolled at multiple practice locations under separate NPIs, a common scenario for group practices and multi-site providers.
- Structured follow-up workflows replace ad hoc email chains. Each payer touchpoint is documented, timestamped, and accessible to anyone on the team.
| ABOUT CREDENTIALLICredentialli is a provider enrollment management platform built for credentialing coordinators, practice administrators, and operations teams that have outgrown their current processes. It consolidates application tracking, document management, payer communication, expirable monitoring, and multi-payer status visibility into a single interface. It does not replace the credentialing work itself, but it removes the operational chaos that surrounds it. |
What Credentialing Delays Cost You (ROI)?
Credentialing is often believed as a compliance and administrative function. The financial framing changes the conversation completely.
The average outpatient provider generates between $1,000 and $1,500 in daily billings. Using a conservative figure of $1,200 per provider per day, every day that provider is not enrolled with a payer signifies potential billings that are either delayed, reduced through out-of-network rates, or lost entirely.
| Scenario | Providers | Daily Billings/Provider | Days Delayed | Revenue at Risk |
| Solo Practice | 1 | $1,200 | 90 days | $108,000 |
| Small Group | 5 | $1,200 | 60 days | $360,000 |
| Mid-Size Practice | 15 | $1,200 | 45 days | $810,000 |
| Multi-Location Group | 30 | $1,200 | 30 days | $1,080,000 |
These figures represent revenue overdue or at risk, not essentially total revenue lost. Some of it may be recoverable through retroactive billing once enrollment is approved, based on the payer’s backdating policy. But much of it, mainly for Medicaid patients and payers that do not backdate, is simply gone.
For group practices bringing on multiple providers at once, the exposure compounds quickly. A 15-provider group experiencing average delays of 45 days per provider is looking at over $800,000 in at-risk revenue per enrollment cycle. That reframes the question from whether to invest in better credentialing workflows to how much revenue loss justifies the delay.
| FRAMINGCredentialing is not a paperwork problem. It is a revenue access problem. Every day without enrollment is a day that revenue is blocked. The question is not whether to optimize the process. The question is how much more delay the practice can afford. |
Frequently Asked Questions
Q1. How long does credentialing take with insurance companies?
Most commercial insurance payers complete credentialing within 60 to 120 days. Medicare enrollment usually takes 60 to 90 days, while Medicaid timelines vary by state. When accounting for documentation, verification, payer review, and enrollment processing, the full provider credentialing timeline typically ranges from 90 to 150 days for most practices.
Q2. What is the difference between credentialing and enrollment?
Credentialing verifies a provider’s qualifications, including licenses, education, certifications, and work history. Enrollment is the process of registering and contracting the provider with an insurance payer network. Although different, both processes work together during provider onboarding and are often managed simultaneously as part of the overall credentialing workflow.
Q3. Can a provider bill while credentialing is in progress?
In most cases, providers cannot bill as in-network until credentialing and enrollment are fully approved. Some payers allow retroactive billing based on the application submission date, while others do not. Practices should confirm each payer’s policy beforehand to avoid denied claims, delayed reimbursements, or unexpected billing complications during enrollment.
Q4. How often is re-credentialing required?
Most insurance payers require re-credentialing every two to three years. Providers must also maintain active licenses, DEA registrations, board certifications, and malpractice coverage. Missing renewal deadlines can delay reimbursements or suspend network participation. Practices that proactively monitor expiration dates reduce compliance risks and avoid interruptions in billing privileges.
Q5. What is CAQH and why does it matter?
CAQH ProView is a centralized provider database used by a number of insurance payers during credentialing and enrollment. Providers upload credentials once, allowing authorized payers to access the information directly. Maintaining an updated and re-attested CAQH profile every 120 days is necessary, as expired profiles often create avoidable enrollment delays.
Q6. What is an NPI and how does it affect credentialing?
An NPI, or National Provider Identifier, is a unique 10-digit number assigned to healthcare providers and organizations in the US. Individual clinicians use Type 1 NPIs, while organizations use Type 2 NPIs. Both are essential for payer enrollment, billing, and credentialing, particularly when providers work across several practice locations.
Stop Managing Credentialing Through Spreadsheets
The credentialing timeline itself is outside your control. What happens around it is not. How well applications are prepared, how consistently payers are followed up with, how quickly expirables are caught, how clearly enrollment status is tracked across dozens of providers and payers. All of that is manageable.
Credentialli is built for credentialing coordinators, practice administrators, and operations teams that have expanded their current processes. It unites the entire provider enrollment workflow into a single structured interface: application tracking, document management, payer communication, expirable monitoring, and multi-payer status visibility, all from one place.
Practices using Credentialli report less rejected applications, quick response times on payer deficiencies, and significantly reduced time-to-enrollment across their provider rosters.
| CREDENTIALLISee How Credentialli WorksSchedule a demo and see how practices are reducing credentialing delays and closing enrollment gaps faster.Schedule a Demo app.credentialli.cominfo@techmatter.co+1 (781) 667-5321 |